You and your partner have been talking about starting a family.
You have done the research.
You have Googled everything from “IVF for lesbian couples” to “shared motherhood IVF.”
And somewhere in the middle of all that searching, you landed on “reciprocal IVF.”
It feels right. It sounds beautiful, actually.
But the details? Still a little fuzzy.
That is exactly why this blog exists.
By the time you finish reading this, you will know exactly how reciprocal IVF works, what happens at every step, how long the whole thing takes, and what it genuinely feels like for both of you.
Let’s get into it.
So, what exactly is reciprocal IVF?

Here is the simplest way to understand it.
One partner provides the eggs.
Donor sperm fertilizes those eggs in a lab.
The other partner carries the pregnancy.
That is the heart of it.
Both of you are involved. Both of you are connected to this baby. One of you contributes the genetic material. The other grows and nurtures the baby inside her body.
That is why so many couples call it shared motherhood. Because that is exactly what it is.
It is not one partner’s journey. It is yours. Together.
Why do so many couples choose reciprocal IVF?

Because it is collaborative in a way that most fertility options are not.
Both of you have a biological role in this pregnancy. The egg-providing partner passes on her genetics. The carrying partner shares her body, her blood, her heartbeat. The baby grows inside her for nine months.
That shared involvement creates a connection that many couples find deeply meaningful. Not just medically, but emotionally.
And unlike traditional IVF where one person handles most of the process, reciprocal IVF allows both partners to participate in creating the pregnancy together.
“Okay, but how do doctors decide who does what?”
Great question. And we will get to that in Step 1.
First, let me walk through the reciprocal IVF process step by step.
Reciprocal IVF step by step process
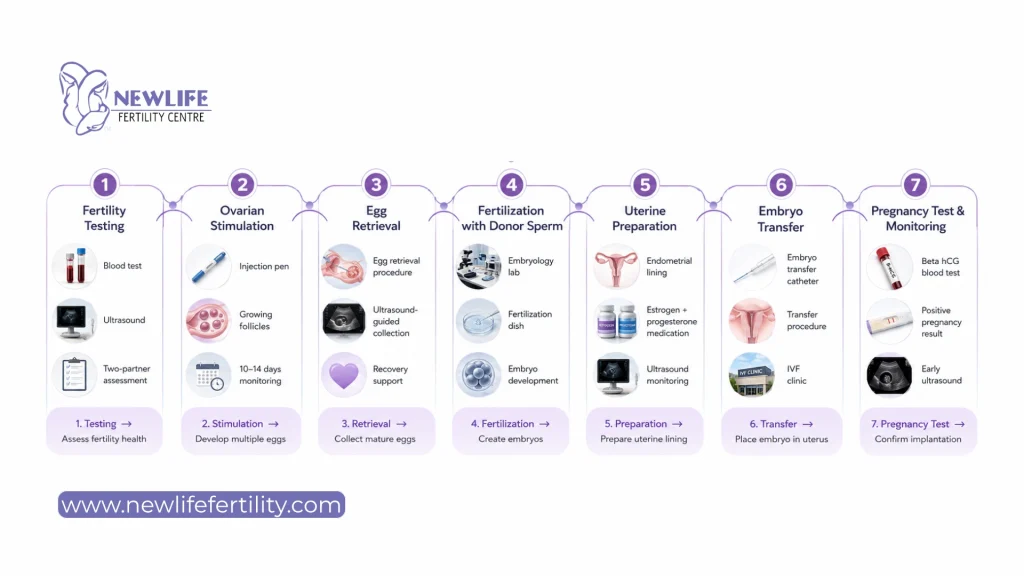
Step 1: Fertility testing for both partners
Before anything else, both partners go through a full round of fertility testing.
Why both?
Because the doctor needs to understand the full picture before making any recommendations.
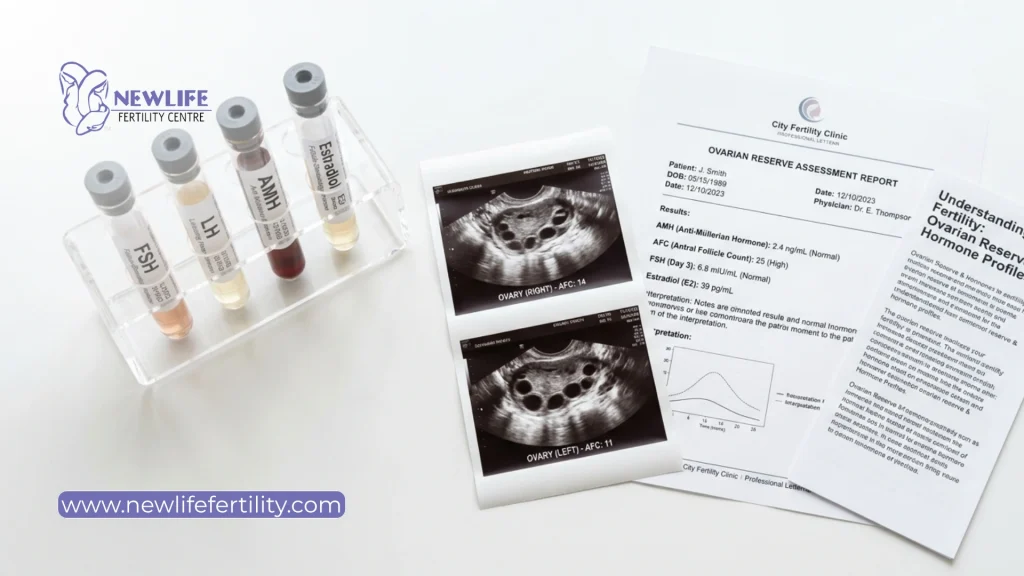
For the partner providing the eggs, doctors check:
→ Hormone levels including AMH, FSH, and estradiol
→ Antral follicle count via ultrasound to assess ovarian reserve
→ Overall egg quality indicators
For the partner who will carry the pregnancy, doctors check:
→ The shape and health of the uterus
→ How well the uterine lining responds to hormones
→ Any conditions that could affect implantation
Both partners also go through infectious disease screening. This is standard practice in any IVF process and nothing to worry about.
How do doctors decide who provides eggs and who carries them?
This is one of the very first questions couples bring into their consultation.
The honest answer: it is a combination of medical factors and personal preference.
Doctors look at age, egg quality, uterine health, and each partner’s medical history. But your own wishes matter just as much. If both of you have strong medical profiles, the decision can be as personal as “who feels more strongly about carrying?”
Some couples walk in already knowing. Others need a little guidance. Either way, your care team will help you figure it out.
Step 2: Ovarian stimulation and fertility medications
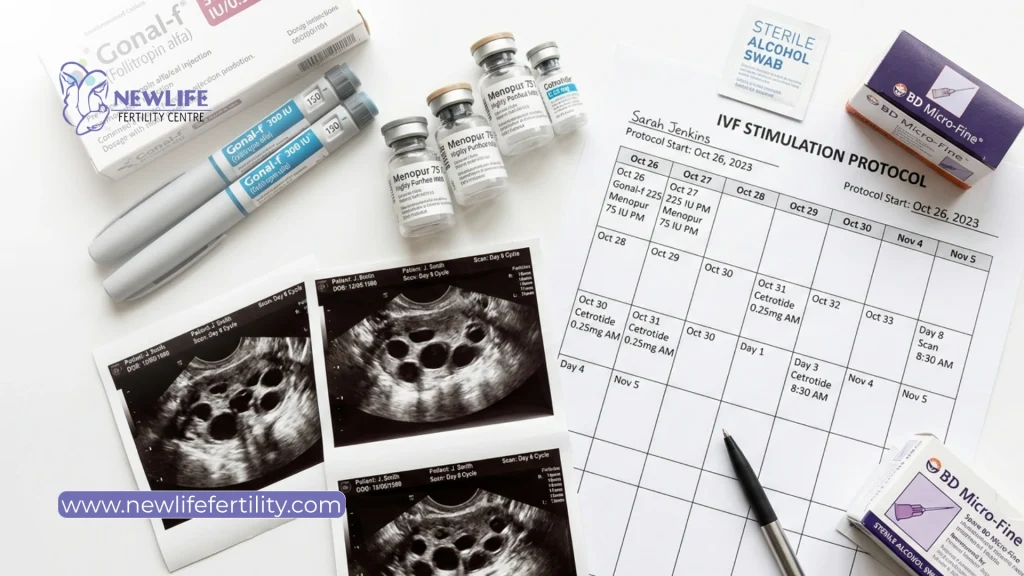
Once it is clear who will provide the eggs, that partner begins the stimulation phase.
This is where the body is gently encouraged to produce more than one egg in a single cycle.
Normally, the body produces one egg per month. In reciprocal IVF, the goal is to produce multiple eggs at once, giving the lab more options and increasing the chances of creating healthy embryos.
How does it happen?
Daily hormone injections.
Your doctor will prescribe a personalized medication protocol. Most injections are self-administered in the abdomen or thigh. It sounds more intimidating than it actually is. Most people get comfortable with it by day two or three.
How long does this stage take?
Usually 10 to 14 days.
During this time, you come in for regular monitoring appointments so the doctor can track how the follicles are growing. Think of follicles as tiny homes where eggs develop inside the ovaries.
What does this phase feel like?
A little uncomfortable at times, but very manageable for most people.
Common experiences include:
→ Bloating, especially toward the end of stimulation
→ Mild mood swings from the hormone changes
→ A sense of fullness or tenderness in the lower abdomen
Most people describe this phase as tiring but exciting. Because at the end of it, real embryos are in the making.
Step 3: Egg retrieval procedure
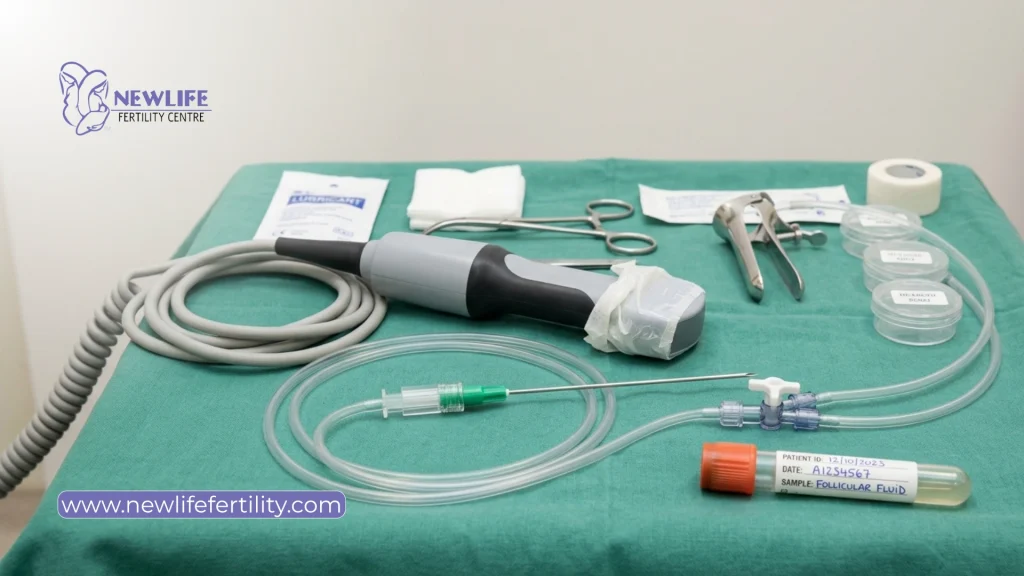
This is the day the eggs are collected.
Egg retrieval is a minor surgical procedure done under sedation. You will be comfortable throughout. You will not feel anything during the actual procedure.
Here is what happens:
A doctor uses a thin needle guided by ultrasound to carefully collect the mature eggs from the follicles. The whole process takes about 20 to 30 minutes from start to finish.
What does recovery look like?
Plan to rest for the rest of the day after retrieval.
Most people experience mild cramping and some bloating afterward, similar to period cramps. This usually settles within 24 to 48 hours. A couple of easy days is typically all you need before feeling back to normal.
And while the egg-providing partner is recovering, the lab has already started doing its part.
Step 4: Fertilization with donor sperm

Now the eggs meet the sperm.
In the lab, the retrieved eggs are fertilized using donor sperm that has been carefully selected and screened. There are two approaches to fertilization:
→ Standard IVF: Sperm and eggs are placed together in a dish and fertilization happens naturally.
→ ICSI (Intracytoplasmic Sperm Injection): A single sperm is injected directly into each egg. This approach is often recommended when higher fertilization rates are needed.
Your clinic will advise which method makes the most sense for your situation.
After fertilization, the embryos go into an incubator and are monitored closely. Over the next three to five days, they develop from a single fertilized cell into what is called a blastocyst. This is the stage most clinics aim for before transfer.
Not every fertilized egg will reach the blastocyst stage. That is completely normal. Your embryologist will give you regular updates throughout this process.
Step 5: Preparing the carrying partner for embryo transfer

While the embryos are growing in the lab, the partner who will carry the pregnancy begins her own preparation.
This involves taking hormone medications, starting with estrogen and then adding progesterone, to prepare the uterine lining for the embryo.
Think of it like preparing the most welcoming environment possible for the embryo to arrive into.
Before the transfer is scheduled, the doctor does an ultrasound to check:
→ Endometrial thickness
→ Hormone levels to confirm the body is responding well
This preparation phase typically runs at the same time as the embryos are developing in the lab, so both processes happen in parallel.
Step 6: Embryo transfer procedure

This is the moment both of you have been working toward.
Embryo transfer is a simple, quick, and calm procedure. No sedation required. Most people describe it as similar to a smear test, mildly uncomfortable but not painful.
The doctor uses a thin, flexible catheter to gently place the embryo into the uterus. The whole appointment usually takes about 10 to 15 minutes.
What happens after transfer?
The carrying partner continues with hormone medications to support the uterine lining.
Your doctor will give guidance on activity. In most cases, there is no need for strict bed rest. Light activity is fine. Avoid anything very strenuous for a few days.
And then comes the part most people find the hardest.
The waiting.
Two weeks after the transfer, there will be a blood test to check for pregnancy. Fourteen days is a long time when you are this invested in the outcome. Give yourselves permission to feel every emotion during this stretch. It is completely understandable.
Step 7: Pregnancy testing and early monitoring

Two weeks after the embryo transfer, the carrying partner has a beta hCG blood test.
This test tells you whether the embryo has implanted successfully.
A positive result and rising hCG levels are a very encouraging sign. Your clinic will typically test twice, a few days apart, to confirm the levels are increasing as expected.
If the result is positive, the next milestone is an early ultrasound. This usually happens around six to seven weeks and is one of the most emotional moments of the entire process.
Your fertility clinic will stay closely involved in the early weeks of pregnancy before transitioning your care to an OB-GYN.
Reciprocal IVF timeline: How long does reciprocal IVF take?

This is one of the first things every couple wants to know.
A typical reciprocal IVF cycle takes around 6 to 10 weeks from the initial consultation to the pregnancy test.
That said, every timeline is slightly different. Your specific medication protocol, how both partners’ bodies respond, and whether you do a fresh or frozen transfer will all affect the overall timeframe.
Here is a rough week-by-week guide to help you plan:
Week 1: Consultation and fertility testing for both partners.
Weeks 2 to 3: Ovarian stimulation for the egg-providing partner, with regular monitoring appointments.
Week 4: Egg retrieval, fertilization with donor sperm, and embryo development in the lab.
Week 5: Embryos continue developing in the lab. The carrying partner begins uterine preparation with hormone medications.
Weeks 5 to 6: Embryo transfer, depending on whether a fresh or frozen transfer is planned.
Two-week wait: Blood test for pregnancy.
What can delay the reciprocal IVF process?
Sometimes the timeline stretches a little longer, and that is not at all unusual.
Common reasons for a longer cycle include:
→ Additional screening results that need follow-up before moving forward
→ A decision to do a frozen embryo transfer instead of a fresh one
→ Hormonal adjustments if the carrying partner’s lining needs more time to prepare
→ Preimplantation genetic testing (PGT), which adds extra lab time before transfer
None of these things are setbacks. They are the clinic making sure conditions are as optimal as possible before the most important step.
Reciprocal IVF vs traditional IVF

A lot of couples researching fertility treatments wonder how reciprocal IVF is different from traditional IVF.
The medical process itself is actually very similar. The biggest difference is who participates in each stage.
In traditional IVF, one person usually goes through both egg retrieval and pregnancy.
In reciprocal IVF, those roles are shared between both partners.
One partner provides the eggs. The other carries the pregnancy.
That shared involvement is what makes reciprocal IVF feel especially meaningful for many same-sex female couples. Both partners play a direct role in creating and carrying the pregnancy journey together.
What does the reciprocal IVF process feel like?

Not just physically. Emotionally too.
For the egg-providing partner
The stimulation phase is the most physically intense part. Daily injections become a routine, and most people find they adjust faster than expected. Retrieval day is quick and over before it feels real.
But the emotional experience? That is harder to put into words.
Knowing that the eggs you have provided will become the baby your partner carries is a feeling that most people describe as one of the most profound of their lives.
For the carrying partner
The hormone medications are manageable. The transfer itself is calm and quick.
But the two-week wait is where it gets hard.
You have done everything right. You have prepared your body carefully. Now the outcome is out of your hands. Many carrying partners describe this as the most emotionally challenging stretch of the whole process.
Staying connected to your partner during these two weeks makes a real difference. Talk to each other. Hold each other. And give yourselves a lot of grace.
Fresh vs frozen transfer in reciprocal IVF

You may hear your doctor mention fresh transfers and frozen transfers. Here is a clear breakdown.
Fresh transfer
A fresh transfer happens within the same cycle as egg retrieval, usually around five to six days after the eggs are collected. The embryo goes straight from the lab to the uterus without any freezing in between.
Frozen transfer (FET)
In a frozen embryo transfer, the embryos are vitrified and stored for use in a future cycle. The carrying partner then undergoes a separate cycle of uterine preparation before the transfer.
Why do many clinics prefer frozen transfers?
A frozen transfer allows the carrying partner’s body to fully reset after hormone medications. It also gives the clinic more flexibility to time the transfer when the uterus is in the best possible condition.
Research shows frozen transfers can achieve equal or better success rates in many cases.
Your doctor will recommend what makes the most sense for both of you based on your individual response to treatment.
Preparing emotionally for reciprocal IVF

Not enough people talk about this part.
The medical side of reciprocal IVF is well-documented and clearly laid out. But the emotional side is just as real.
Going through fertility treatment as a couple means navigating a lot together at the same time. One partner is managing daily injections and physical symptoms. The other is preparing her body for pregnancy while watching her partner go through stimulation.
Talk to each other constantly
Not just about appointments and medications. About fears, expectations, and emotions too.
Manage expectations together
IVF is hopeful, but it is not a guaranteed outcome. Staying realistic while still hopeful is an important balance.
Build a strong support system
Whether that is family, close friends, LGBTQ+ support groups, or a fertility therapist, having emotional support matters more than most couples expect.
Be gentle with yourselves during the two-week wait
Those 14 days can feel incredibly long. Plan comforting distractions, rest when needed, and remind yourselves that every emotion during this phase is valid.
Ready to understand how reciprocal IVF could work for your journey?
Reciprocal IVF is not just a medical procedure. For many couples, it is one of the most meaningful ways to build a family together.
One partner contributes the eggs. The other carries the pregnancy. Both of you are part of the journey from the very beginning. That shared connection is what makes reciprocal IVF feel so personal and emotionally powerful for many LGBTQ+ couples.
And while the process can feel overwhelming at first, understanding how reciprocal IVF works step by step often makes the journey feel far more manageable and less intimidating.
At NewLife Fertility, we understand that every couple’s path to parenthood looks different. Our team works closely with LGBTQ+ families to create personalized fertility treatment plans while offering clear guidance, emotional support, and compassionate care throughout every stage of the reciprocal IVF process.
Whether you are still exploring your options or already thinking about timelines, donor sperm selection, or embryo transfer, you do not need to figure everything out on your own.
Book your free consultation with NewLife Fertility today and speak with a fertility specialist who can help you understand what your next steps could look like.
Frequently asked questions couples ask before starting reciprocal IVF
Yes, and that is the whole point of reciprocal IVF. One partner contributes her genetics through the egg. The other shares her body by carrying and growing the baby for nine months. Both of you are part of this child’s story from the very beginning.
Yes. Reciprocal IVF uses the same well-established protocols as traditional IVF. Both partners are thoroughly evaluated before treatment begins to confirm they are good candidates. The safety profile is well-documented and widely practiced around the world.
It varies by clinic and by how your body responds to medication. During the stimulation phase alone, you can expect monitoring appointments every two to three days. Your clinic will give you a clear schedule upfront so you can plan both your calendars around it.
It absolutely can. Many couples succeed on their first cycle. Success depends on several factors including age, egg quality, and embryo development. Your doctor will give you a realistic and honest picture based on your specific profiles, not a generic one.
This varies widely. The number of eggs retrieved, how many fertilize successfully, and how many develop to blastocyst stage all play a role. Having multiple good-quality embryos is always the goal because it gives you more attempts if you need them. Extra embryos can be frozen for future use.